@ARTICLE{9720240,
author={Sharma, Manuja and Lee, Lauren K. and Carson, Matthew D. and Park, David S. and An, Se W. and Bovenkamp, Micah G. and Cayetano, Jess J. and Berude, Ian A and Xu, Zheng and Sadr, Alireza and Patel, Shwetak N. and Seibel, Eric J.},
journal={IEEE Transactions on Biomedical Engineering},
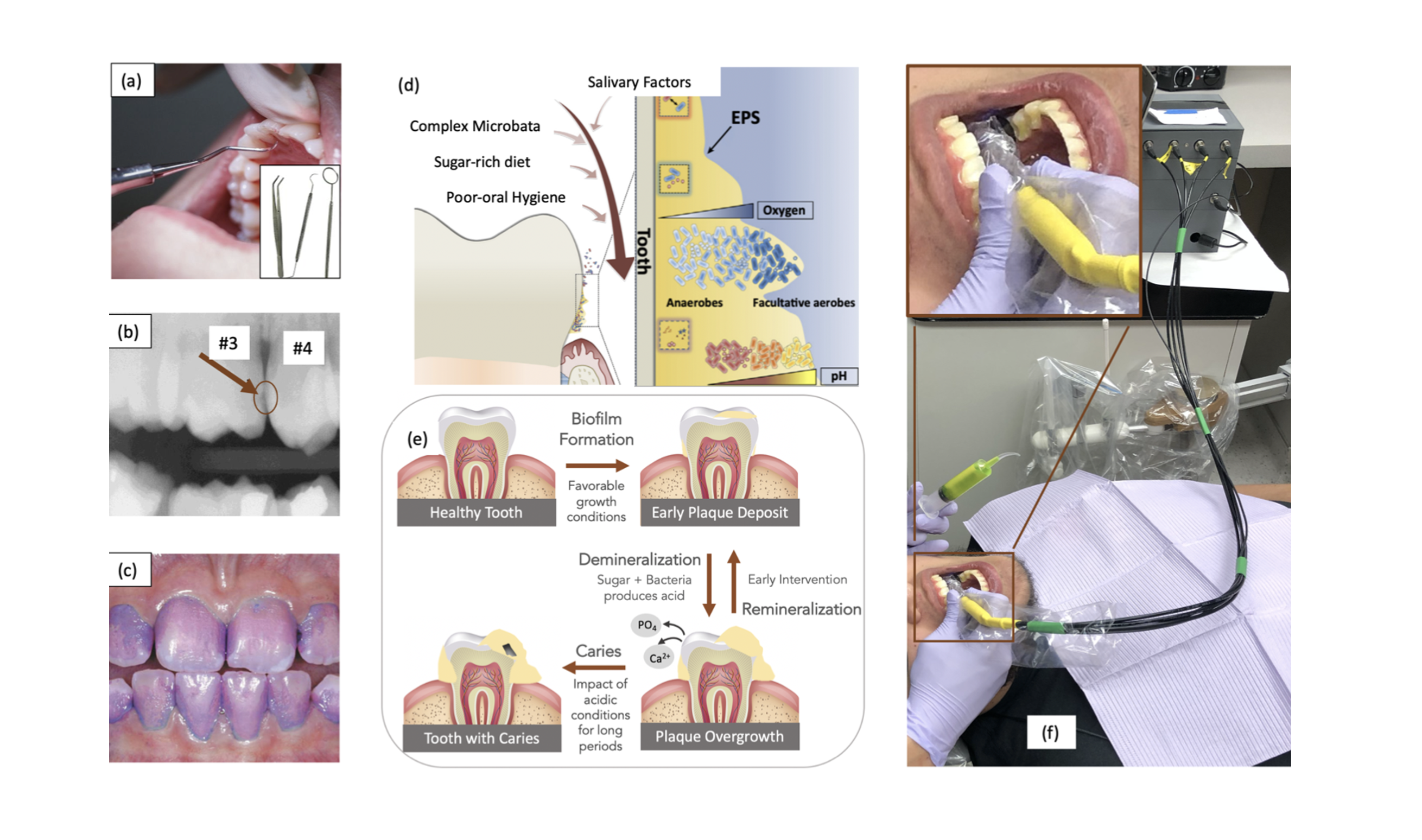
title={O-pH: Optical pH Monitor to Measure Oral Biofilm Acidity and Assist in Enamel Health Monitoring},
year={2022},
volume={},
number={},
pages={1-1},
doi={10.1109/TBME.2022.3153659},
}